
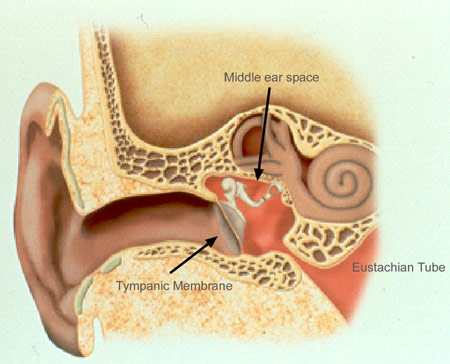
The middle ear and its structures
The middle ear is a hollow chamber in the bone of the skull. It is separated from the outside world by a thin membrane about half-an-inch in diameter, the eardrum. The middle ear area is lined by the same kind of mucous membrane that lines nose and mouth. It is connected to the back of the nose, just above the soft upper portion of the mouth, by a narrow passage called the eustachian tube.
The eustachian tube lies closed until the swallowing movement pulls it open and allows fresh air to enter the middle ear. The fresh air is needed to replace oxygen that has been absorbed by the middle ear lining. The fresh air equalizes the middle ear pressure with the air pressure outside the head. Some people hear this burst of fresh air as a pop or click.
Suspended within the middle ear is a chain of three small bones, the ossicles, which conduct sound vibrations from the eardrum across the middle ear into the fluid-filled inner ear. Inside the inner ear these vibrations are converted to nerve signals that are carried by the auditory nerve to the brain.
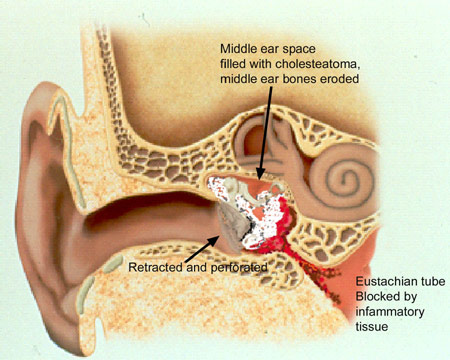
The mastoid bone is an extension of the air space of the middle ear. It is made up of small interconnected air spaces similar to a honeycomb. Its function is not clear, but it is often involved in chronic ear infections. Within it lie the structures of the inner ear responsible for balance and facial expression.
Anatomy of Middle Ear
- Acoustic Neuroma
- Bone-Anchored Hearing Aids
- Cochlear Implants
- Chronic Ear Infections
- Do I Really Need Two Hearing Aids?
- Ear Tubes
- Facial Nerve Weakness
- How Hearing Works
- Hearing Tests
- Tips for Better Hearing
- Meniere's Disease
- Otosclerosis
- Perforations of the Eardrum
- Tinnitus
- Types of Hearing Impairment
- Hearing Aids