
Ear Tubes
Ear tubes are small tubes made out of plastic or metal that are placed into the ear drum to ventilate the middle ear. The middle is that part of the ear between the ear drum and the hard bone surrounding the inner ear. The middle ear is, under normal circumstances, filled with air at the same pressure as the surrounding atmosphere. The pressure is maintained at this normal level by a natural tube called the Eustachian tube. When pressure gets greater or less in the middle ear (for example, when changing altitudes in a plane) the Eustachian tube opens, causing the ears to "pop" and the pressure to equalize. The Eustachian tube also opens during swallowing, chewing, or other jaw movement without producing the pronounced popping sensation.
If the Eustachian tube is not functioning properly, it will not open. This causes the pressure in the middle ear to drop. High negative pressure in the middle ear will draw fluid out from the surrounding tissue and cause fluid to accumulate in the middle ear. This fluid can become infected, setting the stage for recurrent ear infections (otitis media). The infection causes swelling, making it even more difficult for the Eustachian tube to open.
Ear tubes are placed to break this cycle, allowing the ears to drain and to ventilate. The drainage acts in the short term to remove any fluid in the middle ear. The ventilation function is the more important long-term benefit of the tube. With ventilation the lining of the middle ear can return to normal. Since the pressure in now equalized with the surrounding air, there is no accumulation of new fluid, and the chances of additional infections is reduced.
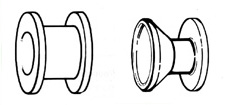
Below are examples of two types of ear tubes. The diameter and the width of each tube is about 3 mm (one-eighth inch).
Ear tubes can also help in those cases in which there is negative pressure in the ear but no fluid. The negative ear can lead to feelings of discomfort or fullness and hearing loss. If the symptoms do not improve with medical treatment, an ear tube can equalize the pressure in this case as well.
In young children the eustachian tube is nearly horizontal. This positioning is felt to interfere with the functioning of the eustachian tube, causing more infections. The muscles that open the eustachian tube are also less well developed in children than in adults.
The ear tubes are put in by making a small incision in the ear drum and inserting the tube through this incision. For adults than can usually be done in the clinic with a local anesthetic.
Since the surgery is very precise, the patient must be very still during the operation. For children the operation is often done in the operating room with a light general anesthetic.

This drawing shows how the ear tube is placed. The incision has been made and the surgeon is just placing the tube into the ear drum, or tympanic membrane. The bone visible just underneath the ear drum is the malleus, also called the hammer. In this diagram, the front of the ear drum is to the right.
There are several different types of tubes. One group of tubes is designed to stay in about 6-9 months and then fall out on their own. Occasionally the tubes will fall out earlier than expected. Less commonly, the tubes will not fall out spontaneously, and must be removed by the physician. The hole used to place the tube heals on its own.
Another type of tube, called a "T" tube (since it is shaped like the letter T) is designed to stay in for a year or more. In most cases it must be removed by the physician.
Adenoids are a collection of lymph tissue (similar to tonsils) in the back of the nose (an area called the nasopharynx). They are important because the Eustachian tube, the pressure equalization tube for the middle ear, opens into the throat right near the adenoids. If the adenoids are enlarged or chronically infected, they can block this opening or, more commonly, serve as a source of infection to travel up the Eustachian tube into the middle ear. The result is recurrent ear infections. Enlarged adenoids can also block the nasal airway, forcing children to breathe through their mouth and causing snoring. In these cases, it is beneficial remove the adenoids at the same time that tubes are placed. Enlarged tonsils do not seem to affect ear infections but can cause problems of their own.
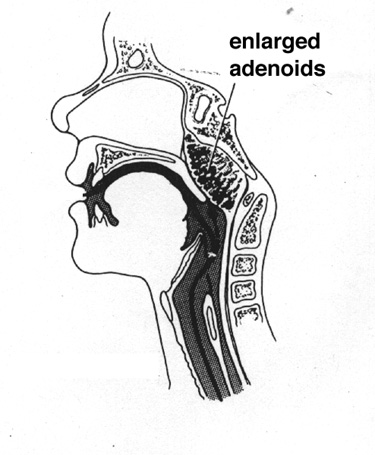
This diagram to the right shows a cross-sectional view of the adenoids. The adenoids lie at the back of the nose in a region called the nasopharynx. When enlarged, the adenoids can interfere with breathing through the nose. They can also harbor bacteria that cause ear infections.
Placement of tubes can sometimes produce a persistent drainage from the ear. This can be treated with ear drops. In some cases (about 1-2% for short-term tubes; greater for the long-term "T" tubes) the hole in the ear drum does not heal. A second operation is sometimes required to patch this hole.
If the tube placement is done with a general anesthetic, there also are risks with administration of the anesthetic. In this day and age, however, general anesthesia is very safe and the patient is very carefully monitored during the procedure. For more information, talk to your anesthesiologist.
Ear tubes are only placed if medical therapy (non-operative treatment) has failed. The question of whether tubes are needed is too complex to answer in format like this web page. It is crucial to carefully discuss these issues and all your questions with your Otolaryngologist. Together you can best decide what treatment is most appropriate.
- Acoustic Neuroma
- Bone-Anchored Hearing Aids
- Cochlear Implants
- Chronic Ear Infections
- Do I Really Need Two Hearing Aids?
- Ear Tubes
- Facial Nerve Weakness
- How Hearing Works
- Hearing Tests
- Tips for Better Hearing
- Meniere's Disease
- Otosclerosis
- Perforations of the Eardrum
- Tinnitus
- Types of Hearing Impairment
- Hearing Aids