
Treatment goals
In unilateral vocal fold paralysis the major problem is usually the inability of one vocal fold to move completely to the midline during speech and swallowing. This can produce a breathy voice and can cause aspiration of food and liquids. There are several different techniques used to treat this movement problem. Most involve using an implant of some type to push the weakened vocal fold closer to the midline. Another option is to attempt to reimplant other nerve fibers into the paralyzed muscles to stimulate them to move again.
Types of treatment
The type of treatment that has become most popular for treatment of unilateral vocal fold immobility is known as vocal fold medialization. This is an operation in which a small implant is surgically implanted inside the larynx to move the immobile fold closer to the midline. There are different materials used for the implant:
- Custom carved silastic (a type of plastic made from silicon)
- Gore-Tex
- Hydroxyapatite (a bone-like material)
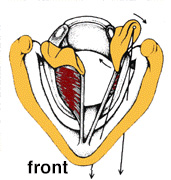
This diagram shows a horizontal cross-section through the larynx with a medialization implant in place. In this diagram, the tan structure is the thyroid cartilage, and the dark red structures are the vocal folds. The implant, shown in blue, is shown pushing the vocal fold on the left closer to the middle.
In most cases, the operation is done using only a local anesthetic, so that the patient is awake. This allows both the surgeon and the patient to assess voice quality during the operation and to adjust the size of the implant to make the voice sound as good as possible.
Important advantages of this operation
- It can be done with the patient awake, so the voice can be assessed throughout the operation.
- It is reversible; the block can be removed if it is later found to be too large or there is some other problem.
- If the nerve to the vocal fold recovers and the fold starts moving again, the block usually does not interfere with normal movement.
Under these circumstances the implant could also be taken out, although this is seldom done if the voice quality is good.
Disadvantages
- It involves a trip to the operating room, with the associated costs.
- The plastic block can become infected or dislodged (these complications are quite rare).
- The block will only move the front two thirds of the vocal fold. The rear one-third will not be affected by this operation.
The arytenoid is a small piece of cartilage that makes up the posterior portion of the vocal cord. The muscles that move the vocal folds are attached to the arytenoids. The medialization procedure described above does not move the arytenoid very well, and some patients will have a breathy voice after the operation due to air leakage in the rear portion of the vocal folds. An arytenoid adduction can be done in these cases.
The term adduction just means movement towards the middle. Since the silicone block or other implant will not move this portion of the vocal fold very well, a different technique is used.
The diagram to the right shows how this procedure works. A suture is first placed through the side of the immobile arytenoid. The stitch is brought to the front and tightened in such a way that the arytenoid swings more toward the midline. The stitch is usually tied to the front of the larynx, as shown in the diagram. This procedure is usually done at the same time as the vocal fold medialization, though it can also be done at a later date. Arytenoid adduction should only be done when there it is certain that the vocal fold function will not occur, since after the operation the fold will not be able to regain any movement.
An arytenoid adduction is more complicated than a simple medialization, and a bit more uncomfortable for the patient if done under a local anesthetic. In some cases a general anesthetic must be used.
Another group of treatment techniques for unilateral vocal fold immobility involves injection of a material into the larynx to push the fold towards the midline. These materials can be used for injection:
- Fat: Fat can be taken from a patient (usually from the abdomen) and injected back into the larynx. Since this is a natural material coming from the patient, there is much less chance of a reaction or infection from the material. However, about 50-70% of the fat is reabsorbed after several months, so the procedure often must be repeated over time.
- Gelfoam: Gelfoam is an absorbable material that can be crushed and injected. It is absorbed slightly more quickly than fat, so it is only a short term solution.
- Teflon: A Teflon paste can be injected to push the fold towards the middle. There are several disadvantages to Teflon which have made the medialization procedure described above more popular. First, it is harder to control exactly where the Teflon finally ends up. The Teflon particles can infiltrate the muscles or lining of the vocal fold, which worsens the natural vibratory function of the vocal fold and produces poor voice quality. Teflon can cause reactions in some people, producing what is called a granuloma. Finally, Teflon is much more difficult to remove than the silicone block and the procedure is therefore less reversible. Also, if nerve recovery eventually occurs and vocal fold function returns after a Teflon injection, the voice may not improve as much as it would if medialization had instead been performed. One advantage of Teflon injection is that, in some cases, it can be injected in the physician's office or clinic, and therefore does not always require a trip to the operating room.
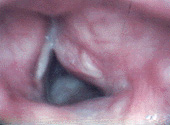
The image to the left shows a Teflon granuloma on the patient's right vocal fold. The vocal fold on the left is normal. Note that the right side is very swollen and inflamed. This exam was made about 6 months after the Teflon injection. By this time the vocal fold had already recovered and was moving normally. However, the voice was very poor. Fortunately, it was relatively easy to remove the Teflon and the patient ended up with a fairly normal voice. In many cases the scarring becomes more fibrotic and voice recovery is not good.